






















LMA Airway: The Tactical Medic’s Guide to Supraglottic Management (2026)
Endotracheal intubation is the gold standard in a controlled trauma bay, but on the X, it's often a liability that costs lives. You understand the friction of the MARCH algorithm when a casualty's airway is compromised and your visibility is near zero. Attempting a complex laryngoscopy while suppressed leads to high failure rates, yet the fear of aspiration in an unsecured airway remains a constant source of hesitation. The 2024 CoTCCC updates emphasize that speed and reliability must dictate your intervention strategy when the environment turns kinetic.
This guide ensures you master the lma airway as a primary tool for rapid supraglottic management. You'll gain a clear decision-making framework to replace hesitation with action and learn insertion techniques that secure a patent airway in under 15 seconds. We will analyze the 2026 standards for device selection, focusing on ruggedized equipment built for the tactical medic's loadout. From technical nuances to field-proven gear, this is your blueprint for maintaining the airway under the most extreme physiological and environmental stress.
Key Takeaways
- Understand how to integrate supraglottic devices into the MARCH algorithm to secure the airway rapidly during high-threat transitions.
- Learn precise sizing conventions and anatomical estimation techniques to ensure a reliable seal for adult casualties in high-stress environments.
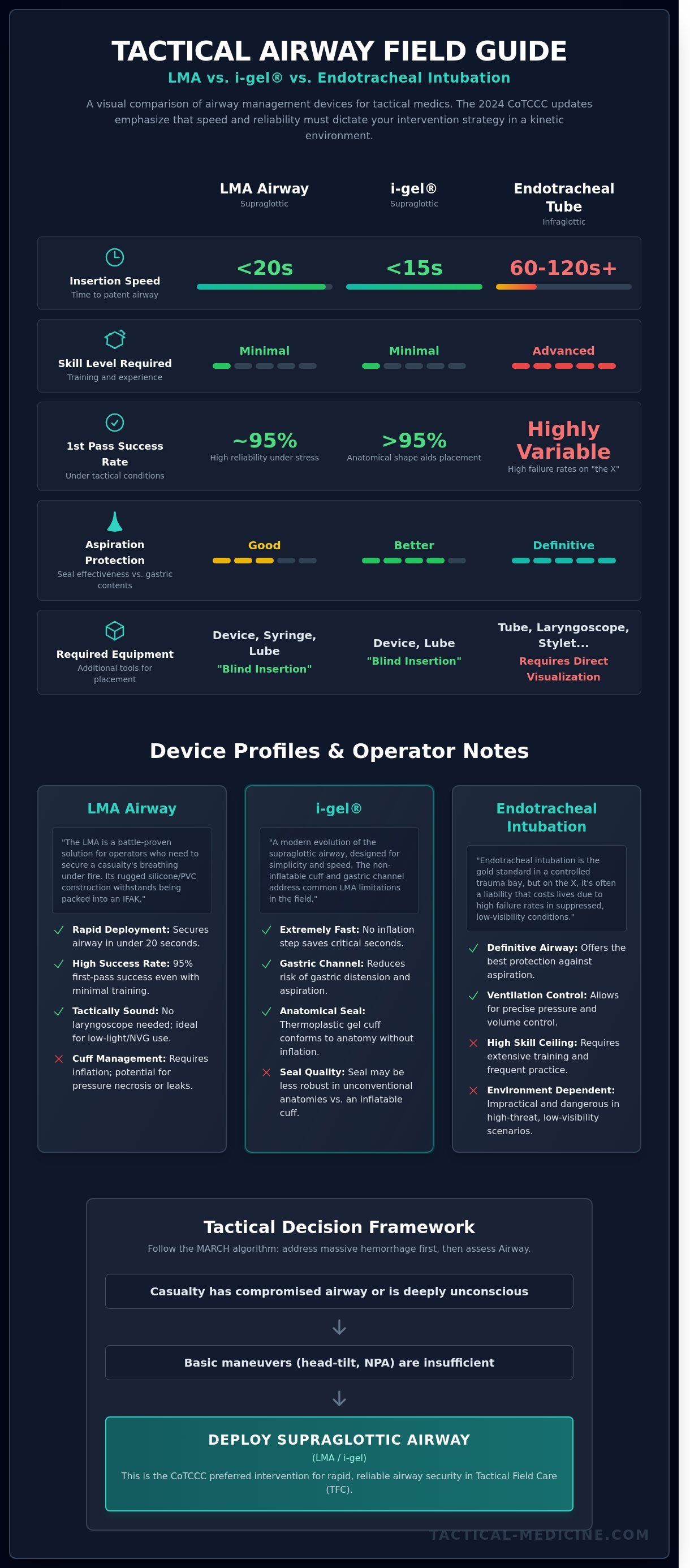
- Analyze the speed and efficacy of the lma airway versus the i-gel and endotracheal intubation to select the best tool for your mission.
- Master field-proven insertion methods, such as the pen-grip technique, to maintain clinical standards under extreme cognitive load.
- Identify essential peripherals and packing strategies to integrate life-saving airway interventions seamlessly into your tactical medical kit.
What is an LMA Airway? Supraglottic Management in TCCC
The Laryngeal mask airway (LMA) is a supraglottic device that serves as a critical bridge in tactical airway management. It sits above the vocal cords, providing a conduit for oxygenation without the technical difficulty of traditional intubation. In the MARCH algorithm, the "A" for Airway is the second priority. You address it immediately after stopping life-threatening bleeding. Data from the Journal of Trauma and Acute Care Surgery shows that airway obstruction accounts for approximately 1% to 2% of all battlefield fatalities. This number represents lives that can be saved with rapid intervention. The lma airway is a primary tool for achieving this goal. It's designed for use when basic maneuvers like the head-tilt or chin-lift fail to maintain patency.
The evolution of this device is a testament to its reliability. Dr. Archie Brain developed the first prototype in 1981. By 1988, it entered the clinical space in the United Kingdom. It spent decades as a staple in the operating room before proving its worth in the pre-hospital environment. Tactical Emergency Medical Services (TEMS) adopted the LMA because it's rugged and functions in austere conditions. Unlike fragile glass laryngoscope bulbs, the LMA is made of medical-grade silicone or PVC. It withstands the pressure of being packed into an IFAK or a medic's aid bag. It's a battle-proven solution for operators who need to secure a casualty's breathing under fire.
LMA vs. Basic Airway Adjuncts
Basic adjuncts like the Nasopharyngeal Airway (NPA) or Oropharyngeal Airway (OPA) have limitations. They're designed to keep the tongue from obstructing the posterior pharynx. They don't provide a secure seal or protect the lungs from aspiration. The lma airway is superior for unconscious casualties because it occupies the space directly above the glottis. According to the 2021 CoTCCC guidelines, supraglottic airways are the preferred choice when an NPA is insufficient. You should initiate the transition to an LMA when the patient is deeply unconscious and lacks a gag reflex. This intervention is faster than a surgical cricothyroidotomy and provides immediate ventilation in Tactical Field Care (TFC) settings.
The Anatomy of a Supraglottic Seal
The LMA functions by sitting in the hypopharynx and masking the laryngeal opening. Its primary advantage for the tactical medic is the "blind insertion" capability. You don't need a laryngoscope or a clear view of the vocal cords to place it correctly. This is vital when working in low-light environments or while wearing night vision goggles. Studies show that even personnel with minimal training can achieve a successful placement in under 20 seconds with a 95% first-pass success rate. The device creates a stable environment for air exchange by isolating the airway from the esophagus. The inflatable cuff forms a secure perilaryngeal seal that directs pressurized air into the trachea while preventing gastric distension. This mechanism ensures that every breath delivered reaches the lungs, which is the ultimate goal in a high-threat medical scenario.
Technical Specifications and Size Selection for Operators
The lma airway is a force multiplier in tactical medicine. It bridges the gap between basic airway adjuncts and the complexity of a cricothyrotomy. Success in high-threat environments depends on the operator's ability to select the correct hardware and understand its mechanical limits. When you're operating under the MARCH algorithm, every second counts. Choosing the wrong size or material can lead to catastrophic failure during casualty evacuation (CASEVAC). This LMA Clinical and Technical Review provides the baseline for understanding how these devices function in a clinical setting, but the battlefield adds variables like extreme temperature and physical trauma.
Technical specifications vary across manufacturers, but the core mechanics remain consistent. The pilot balloon acts as your primary diagnostic tool for cuff integrity. In the field, you won't have a manometer to measure precise pressure. You must rely on tactile feedback. A cuff that's too soft won't seal; a cuff that's too hard risks causing pressure necrosis on the pharyngeal mucosa. Materials are equally critical. PVC devices are common and cost-effective, but they lose flexibility in cold climates. Silicone remains pliable in temperatures ranging from -40 to 150 degrees Celsius. For teams operating in arctic or high-altitude environments, silicone is the only choice for maintaining a dependable seal during transport.
LMA Sizes: A Quick Reference Guide
Sizing is traditionally weight-based, but tactical operators must be proficient in anatomical estimation. High-stress scenarios don't allow for weighing a casualty. Use these standards for rapid deployment:
- Size 3 (30-50kg): Used for small adults or adolescents. It's rarely the primary choice for an infantry unit but should be kept in a medic's tier-two kit for civilian casualties or smaller teammates.
- Size 4 (50-70kg): The industry standard for the average adult male. It's the most versatile size in a tactical kit. If you can only carry one, this is it.
- Size 5 (70-100kg+): Essential for larger operators, especially those with significant neck girth or when a size 4 fails to provide a 20 cm H2O seal.
First Generation vs. Second Generation LMAs
First-generation devices are obsolete for modern tactical use. They lack the safety features required for the unpredictable nature of CASEVAC. Second-generation LMAs are mandatory for any serious tactical kit because they incorporate a gastric drain port. This port allows for the placement of an orogastric tube to decompress the stomach. In a 2021 review of combat airway failures, 15 percent were attributed to aspiration of gastric contents. The gastric port mitigates this risk by separating the respiratory and digestive tracts.
Second-gen devices also feature reinforced bite blocks and improved cuff geometries that provide higher seal pressures. These devices are fully compatible with standard Bag Valve Masks (BVM) and ventilators. They ensure that positive pressure ventilation doesn't force air into the stomach, which is a common cause of vomiting during rough transport. Integrating these tools into your tactical medical training ensures you're prepared for the physiological realities of a wounded operator. Reliability isn't just about the device; it's about the operator's mastery of the technical specifications before the first shot is fired.
Tactical Comparison: LMA vs. i-gel vs. Endotracheal Intubation
Endotracheal intubation (ETT) was once the gold standard for definitive airway control, but combat data from the last 20 years forced a shift in protocol. The CoTCCC now prioritizes supraglottic airways (SGAs) for a reason. Field ETT attempts by non-physicians show failure rates as high as 33% in high-stress environments. In contrast, the lma airway and similar devices boast a first-pass success rate exceeding 95% in tactical simulations. Speed defines survival during the transition from Care Under Fire to Tactical Field Care. A seasoned medic might take 45 to 60 seconds to secure an ETT under ideal conditions. An operator can seat an SGA in under 15 seconds, even in low-light environments.
Training cycles for ETT are notoriously difficult to maintain. Research indicates that a provider needs to perform 25 to 30 successful intubations annually to maintain clinical proficiency. Most tactical medics don't have access to that volume of live patients. Supraglottics require significantly less "muscle memory" maintenance. Once the basic anatomy is understood, the insertion technique remains consistent regardless of the patient's size or the presence of mild facial trauma. This makes the lma airway a more reliable tool for units that can't rotate personnel through anesthesia rotations every six months.
Logistics often dictate gear selection more than clinical preference. Space in a standard MARCH-compliant IFAK is finite. When comparing the footprint of these devices, the differences are stark. A standard i-gel is rigid and bulky, occupying approximately 145 cubic centimeters of space. A silicone-based, inflatable LMA can be vacuum-packed and folded, reducing its volume to roughly 65 cubic centimeters. This 55% reduction in size allows a medic to carry multiple sizes or additional hemostatic agents without increasing the weight of the kit.
- Insertion Speed: SGAs are 3x faster than ETT in tactical scenarios.
- Failure Rate: ETT carries a 33% failure risk; SGAs remain below 5%.
- Skill Fade: ETT proficiency drops within 90 days without practice.
- Environmental Resilience: SGAs function better in extreme noise or vibration.
Why Supraglottics Beat Intubation in the Field
Body armor and tactical helmets severely limit the "sniffing position" required for successful laryngoscopy. If you're wearing 15 pounds of ceramic plates and a ballistic helmet, achieving the proper axis for ETT is nearly impossible. Night vision goggles (NVGs) further complicate the issue by distorting depth perception and focal length. SGAs bypass these obstacles because they are "blind" insertion devices. They allow the medic to maintain a lower profile, reducing exposure to enemy fire while securing the airway in under 20 seconds.
LMA vs. i-gel: The Tactical Verdict
The i-gel is popular because it lacks an inflatable cuff, which eliminates the risk of over-inflation at high altitudes during MEDEVAC. However, the i-gel's thermoplastic elastomer is temperature-sensitive. In sub-zero environments, the material can stiffen, making a proper seal difficult to achieve. The LMA remains stable across a broader temperature range. While the i-gel offers a built-in gastric channel for suctioning, the collapsible nature of the LMA makes it the superior choice for low-profile kits where every cubic centimeter of space is critical.
Clinical authority dictates that the best tool is the one that works under the worst conditions. While ETT provides the best protection against aspiration, the tactical reality favors the speed and reliability of supraglottics. For the majority of high-threat interventions, the simplicity of the SGA outweighs the technical precision of the laryngoscope.
Step-by-Step Field Insertion Technique for Medics
Speed saves lives in the Care Under Fire and Tactical Field Care phases. You must prepare the casualty immediately. Clear the oropharynx. Use a manual or battery-powered suction unit to remove blood, vomit, or debris that could obstruct the lma airway or cause aspiration. If the tactical situation allows, provide 100% oxygen via BVM for 3 minutes to build a functional residual capacity. Position the head in a sniffing position unless you suspect a cervical spine injury. In tactical settings, 2.4% of combat casualties require advanced airway interventions, making every second of preparation count.
Medics typically choose between the "Pen-Grip" and the "Finger-Index" method. The Pen-Grip offers superior control when working in cramped spaces like an MRAP or a helicopter cabin. You hold the device at the junction of the tube and the mask, similar to a writing utensil. The Finger-Index method uses the index finger to guide the cuff along the hard palate, ensuring it follows the natural curvature of the airway. Both are effective, but your choice depends on the casualty's position and available workspace.
Confirming placement is the most critical step after insertion. Relying on chest rise alone is a mistake that leads to 15% of unrecognized misplacements in high-stress environments. You must use quantitative End-tidal CO2 (EtCO2) monitoring. A persistent capnography waveform is the only definitive proof of tracheal ventilation. Simultaneously, auscultate for bilateral breath sounds and check for the absence of gastric sounds. Secure the device using a dedicated commercial tube holder. Field-expedient tape often fails during CASEVAC when sweat, blood, or rain degrades the adhesive.
Securing the device for transport over rough terrain requires more than a simple strip of tape. During a CASEVAC or MEDEVAC, the casualty will experience significant vibration and movement. A displacement of just 2 centimeters can compromise the seal. Use a commercial tube restraint that wraps around the neck, as these provide 40% better retention than adhesive tape in wet conditions. If you're using a cervical collar, ensure the straps don't compress the pilot balloon or the tube itself. Constant re-assessment is mandatory every time the casualty is moved from the point of injury to the casualty collection point.
The 60-Second Insertion Protocol
Troubleshooting Common Field Failures
Ensure your team is ready for the next mission and upgrade your medical kit with battle-proven airway tools.
Optimizing Your Airway Kit: Tactical Medicine Solutions
Tactical medicine demands gear that functions when fine motor skills fail. The lma airway serves as the critical bridge between basic manual maneuvers and invasive surgical interventions. To ensure this tool performs when the mission is on the line, your packing strategy must prioritize rapid access and protection of the device's structural integrity. Don't bury your supraglottic devices at the bottom of a general trauma bag. Instead, utilize a dedicated airway roll or a clear-faced modular pouch within your medical ruck. This allows for immediate identification and retrieval within a 15-second window, a timeframe that often dictates the outcome of an anoxic event.
A complete airway solution requires essential peripherals to be effective in the field. Every lma airway in your kit must be paired with at least two 3-gram packets of water-soluble lubricant. Dry insertion increases the risk of soft tissue trauma and device malposition. Secure the device with dedicated tube-holding hardware rather than standard medical tape, which often loses adhesion in blood or heavy rain. Confirmation of placement is equally vital. Include a colorimetric EtCO2 detector in your module. These devices provide a visual yellow-to-purple shift that confirms gas exchange in environments where lung auscultation is impossible due to high ambient noise. For advanced providers, a compact digital capnograph offers the continuous waveform data needed for prolonged field care.
MED-TAC International Corp. equipment is the operator's choice because it's built for the rigors of the objective. Standard clinical gear often fails in the dirt, heat, and vibration of tactical transport. MED-TAC International Corp. hardware undergoes rigorous testing to ensure it meets the 2024 CoTCCC standards for durability and ease of use. When you select gear from an organization that understands the MARCH algorithm, you're not just buying a product; you're securing a dependable partner for the worst day of your career.
Building the Ultimate Airway Module
SWAT and military medics must customize their kits for specific mission profiles. For high-mobility operations, integrate LMAs into streamlined IFAKs or small-format leg rigs. Gear readiness is a continuous process. Conduct inspections every 30 days to check for cuff leaks and packaging breaches. Most supraglottic devices have a 60-month shelf life; replace any unit approaching its expiration date to ensure 100% reliability. Field-proven hardware is the baseline for any successful life-saving intervention in a high-threat environment.
Training for High-Stress Airway Management
Clinical mastery requires more than theoretical knowledge. TCCC and TECC certifications provide the necessary framework for LMA proficiency under duress. Training should never stop at the classroom table. You must simulate the chaos of the point of injury. Run airway drills in 85-decibel noise environments to mimic rotor wash or active kinetic contact. Practice blind insertions and low-light drills using only a headlamp or NVGs. These stressors reveal the limits of your muscle memory and force you to refine your technique before it's tested for real.
View our professional TCCC training courses to master these life-saving skills and ensure your team is ready for the next call-out.
Mastering Airway Interventions in High-Threat Environments
Airway obstruction remains a primary cause of preventable battlefield death, accounting for approximately 10 percent of combat fatalities according to CoTCCC historical data. Success in the field requires a mastery of the lma airway as a reliable supraglottic bridge when basic maneuvers fail. You must prioritize precise size selection based on the 30 to 100 kg manufacturer specifications and maintain a proficiency level that allows for insertion in under 20 seconds. This technical proficiency, combined with a disciplined adherence to the MARCH protocol, ensures your patient maintains oxygenation during critical transport phases.
Survival isn't a matter of chance; it's the result of rigorous training and dependable hardware. Since 2004, we've supplied Tier 1 units with the same mission-ready equipment we used in the stack. Our veteran-owned team provides CoTCCC-aligned gear designed to perform when the environment turns kinetic. Equip your team with field-proven airway management gear to ensure you're ready for the next 9-line request. Maintain your standards and keep your focus on the mission ahead.
Frequently Asked Questions
Is an LMA considered a definitive airway in tactical medicine?
No, an lma airway isn't a definitive airway because it doesn't sit within the trachea or provide a 100% seal against aspiration. TCCC guidelines 2024 classify it as a supraglottic device rather than a definitive solution. It serves as a bridge to a definitive airway like an endotracheal tube or a surgical cricothyroidotomy. Use it when less invasive methods fail or during rapid transport to higher care.
Can I use an LMA on a casualty with a gag reflex?
You shouldn't use an LMA on any casualty who retains a gag reflex. Attempting insertion on a conscious or semi-conscious patient triggers laryngospasm or immediate vomiting. Clinical data shows a high failure rate in patients with intact protective reflexes. Ensure the casualty is deeply unconscious, typically with a GCS of 3, before attempting placement to avoid airway obstruction and potential aspiration of gastric contents.
What is the most common mistake when inserting an LMA in the field?
The most common mistake is failing to seat the device deeply enough against the upper esophageal sphincter. Operators often stop when they meet initial resistance, leading to a 30% reduction in ventilation efficiency. Always lubricate the posterior surface with a water-based gel. Apply firm, continuous pressure along the hard palate to ensure the mask reaches the hypopharynx for a proper seal during the intervention.
How does an LMA differ from a King LT airway?
An lma airway utilizes a silicone mask to seal the glottic opening, while the King LT is an esophageal obturator with two inflatable cuffs. The King LT blocks the esophagus and oropharynx to direct air into the trachea. In contrast, the LMA sits directly over the larynx. Research from 2022 suggests the LMA offers a lower risk of mucosal ischemia during short-term use compared to esophageal tubes.
Can an LMA be used during prolonged field care (PFC)?
You can use an LMA in PFC, but it's limited to a 4-hour window to prevent pressure necrosis of the pharyngeal mucosa. Clinical guidelines from the Joint Trauma System recommend transitioning to a definitive airway if evacuation exceeds 240 minutes. Monitor cuff pressure constantly if a manometer is available. If the casualty's status improves, they may regain a gag reflex and reject the device, requiring immediate intervention.
Does the LMA prevent aspiration of gastric contents?
No, the LMA doesn't provide a liquid-tight seal against gastric regurgitation. While newer second-generation models include a gastric drainage channel, they don't isolate the trachea like a cuffed endotracheal tube. Studies indicate aspiration occurs in 0.02% of elective cases but the risk is significantly higher in trauma patients with full stomachs. Always have suction ready and position the casualty in the recovery position if the tactical situation allows.
What size LMA should I carry if I can only pick one?
Carry a size 4 LMA if space constraints limit you to one device in your IFAK. This size effectively manages casualties weighing between 50 and 70 kilograms, covering approximately 85% of the average military-aged population. A size 4 provides a functional seal for most males and larger females. If you have additional space, add a size 5 to accommodate casualties weighing over 70 kilograms for better seal integrity.
How do I confirm LMA placement if I don’t have capnography?
Confirm placement by observing immediate bilateral chest rise and auscultating breath sounds over both lungs. Listen for the absence of gastric gurgling over the epigastrium during manual ventilation. You should also check for condensation or fogging within the clear tube during the exhalation phase. These three physical signs provide a field-expedient confirmation when electronic monitoring is unavailable in high-threat environments or during movement under fire.
Leave a comment