

















Bag Valve Mask (BVM): The Tactical Operator’s Guide to Manual Ventilation
A 2021 study published in Prehospital Emergency Care revealed that 45% of medical providers inadvertently hyperventilate patients during manual resuscitation. In a high-threat environment, this technical failure leads to increased intrathoracic pressure and decreased cerebral perfusion. You understand that managing the Airway component of the MARCH algorithm is a zero-fail mission. The struggle to maintain a consistent mask seal while managing equipment bulk in a cramped vehicle or a dark hallway is a reality every operator faces.
This guide ensures you master the clinical mechanics and tactical application of the bag valve mask to maintain patent ventilation under extreme stress. We'll provide the specific protocols needed to prevent gastric inflation and optimize oxygenation without compromising your security posture. You'll learn the exact criteria for selecting a rugged, collapsible BVM for your trauma bag and the troubleshooting steps required to fix a failing seal in seconds.
Key Takeaways
- Integrate the bag valve mask into the 'Airway' phase of the MARCH algorithm to provide effective positive pressure ventilation.
- Master critical field techniques, including the E-C clamp seal and trauma-specific positioning, to ensure a patent airway under stress.
- Identify and mitigate common failure points such as gastric inflation and compromised seals caused by facial trauma or debris.
- Optimize your medical loadout by selecting mission-capable hardware that balances durability with the spatial constraints of an IFAK or medic bag.
The Role of the Bag Valve Mask in Tactical Airway Management
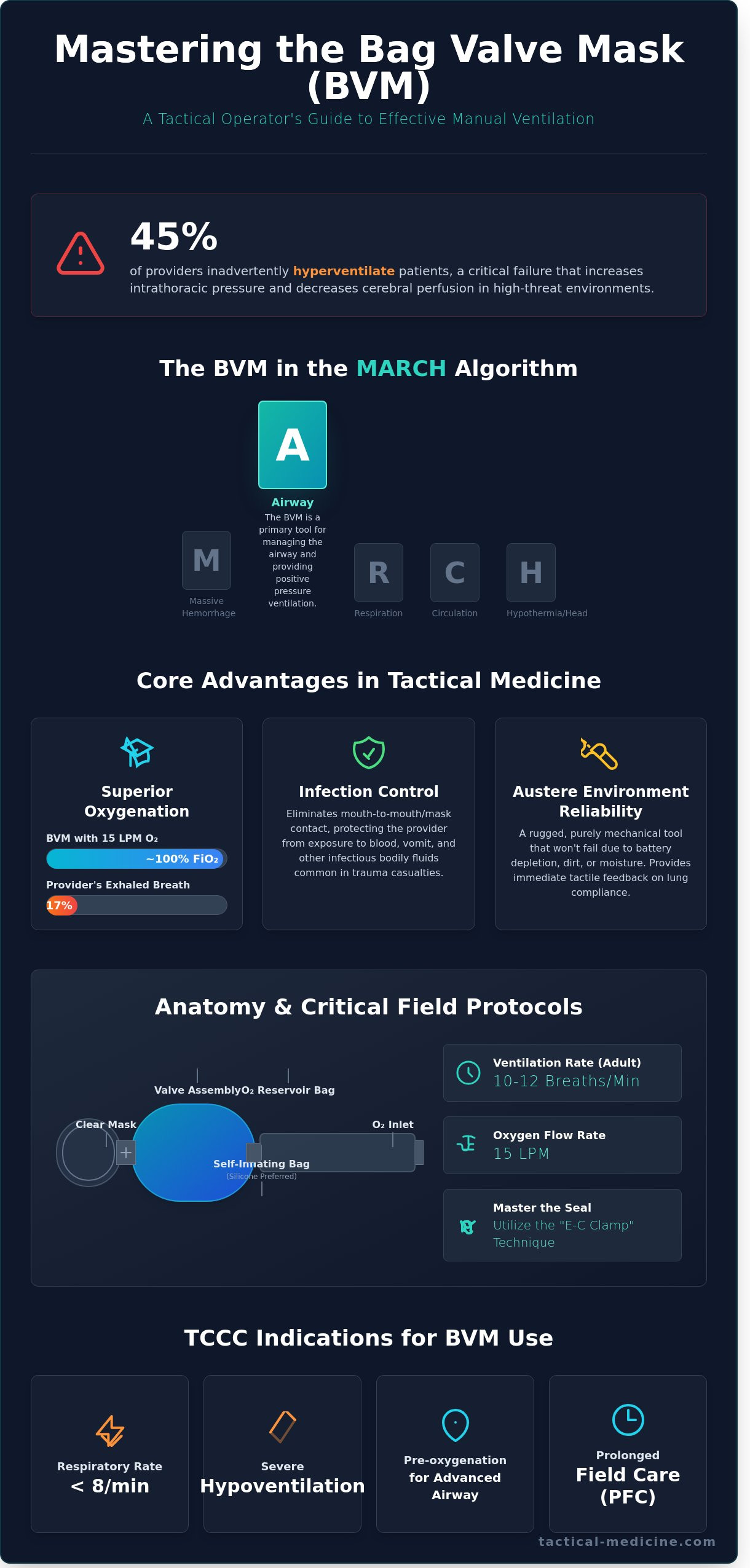
The Bag valve mask (BVM) is the standard manual resuscitator used to provide positive pressure ventilation in high-threat environments. Within the MARCH algorithm, the BVM is a critical component of the Airway (A) phase. While massive hemorrhage remains the primary focus of initial care, respiratory failure is a leading cause of preventable death on the battlefield. The bag valve mask allows an operator to manually deliver oxygen to a casualty who can no longer breathe effectively on their own. It’s a bridge between the point of injury and definitive surgical care. The primary mission of this device is to maintain oxygenation and prevent hypoxia when spontaneous respiration fails or becomes inadequate to support life.
BVM Indications in TCCC
Tactical Combat Casualty Care (TCCC) 2024 guidelines emphasize specific triggers for manual ventilation. Primary blast injuries often result in traumatic brain injuries (TBI) that suppress the central nervous system, leading to respiratory arrest. If a casualty presents with a respiratory rate below 8 breaths per minute or shows signs of severe hypoventilation, the BVM is the immediate intervention. In Prolonged Field Care (PFC) scenarios, where evacuation times exceed the 2-hour standard, the BVM is used to assist ventilations during patient stabilization or while managing casualties with decreased levels of consciousness. It’s also vital for pre-oxygenation before advanced airway procedures like endotracheal intubation or cricothyroidotomy.
Why Tactical Medics Prioritize the BVM
- Infection Control: The BVM eliminates the need for mouth-to-mouth or mouth-to-mask contact. This protects the provider from exposure to blood, vomit, and other infectious bodily fluids common in trauma cases.
- Oxygen Concentration: When connected to a portable oxygen source at 15 liters per minute, a BVM can deliver nearly 100% oxygen. This is significantly more effective than the 16% to 17% oxygen concentration found in a provider's exhaled breath.
- Tactical Reliability: Automated ventilators often fail in austere conditions due to battery depletion or mechanical damage from dirt and moisture. The BVM is a rugged, purely mechanical tool. It provides the medic with immediate tactile feedback regarding lung compliance, which is essential for identifying conditions like tension pneumothorax or airway obstructions in the field.
Anatomy of a Life-Saving Device: BVM Components and Mechanics
The bag valve mask is not a single tool; it's a modular system designed for rapid, manual ventilation. The self-inflating bag acts as the engine of the device. It must provide immediate recoil to maintain a consistent ventilation rate of 10 to 12 breaths per minute for adult casualties. Tactical operators favor medical-grade silicone bags over standard PVC because they resist permanent deformation when packed tightly in a kit for extended periods. This durability ensures the bag returns to its original shape instantly, even after thousands of compressions in high-stress environments.
The oxygen reservoir is a critical component that often goes underutilized in the field. When connected to a 15 liter per minute (LPM) oxygen source, the reservoir allows the operator to deliver a Fraction of Inspired Oxygen (FiO2) approaching 1.0. Without the reservoir, the FiO2 drops to approximately 0.40, which is insufficient for casualties suffering from severe hemorrhagic shock or pulmonary contusions. Mastering the BVM ventilation technique ensures these mechanics translate into effective oxygenation for the casualty.
The Valve System and PEEP Integration
The valve assembly prevents the patient from rebreathing exhaled gases by using a series of one-way gates. A duckbill or disk valve directs the volume into the patient's lungs during compression and closes during the bag's refill phase. A PEEP valve is a non-negotiable addition to your bag valve mask setup when managing blast-related lung injuries. It maintains a set level of pressure, typically 5 to 10 cm H2O, during the expiratory phase to prevent alveolar collapse. This is vital during long-range tactical transport where lung recruitment is difficult to maintain.
Pediatric BVMs include a pressure-release valve, often calibrated to 35 or 45 cm H2O. This "pop-off" mechanism is a safety feature that mitigates the risk of barotrauma in smaller, more fragile lung structures. Operators must know how to override this valve if the casualty's lung compliance is so poor that higher pressures are required to achieve chest rise.
Mask Design and Seal Integrity
Seal integrity is the primary point of failure in manual ventilation. Operators should utilize clear masks to monitor for gastric regurgitation or secretions that could lead to aspiration. The mask features a 22mm female connector that fits standard bag units, while the 15mm internal diameter allows for direct connection to an lma airway or endotracheal tube. This universal sizing ensures compatibility across different tiers of airway management.
In environments where temperatures drop below -10°C, standard PVC masks lose flexibility and fail to conform to the casualty's face. Silicone components remain pliable, ensuring a seal is maintained even in arctic conditions. The inflatable cuff on the mask's rim should be checked regularly; a mask with a slow leak is useless when trying to ventilate against high airway resistance. Ensure your kit is stocked with mission-ready ventilation tools before your next deployment.
Step-by-Step Guide: Effective BVM Ventilation in the Field
Proper positioning dictates the success of manual ventilation. For non-trauma casualties, utilize the sniffing position by extending the neck and elevating the head. Trauma cases require a modified jaw-thrust to prevent spinal cord injury while maintaining airway patency. You must maintain this position throughout the intervention. Once positioned, monitor for visible chest rise and fall with every breath. Deliver 500 to 600 mL of air over one second. Follow a strict squeeze, release, release rhythm to maintain a rate of 10 to 12 breaths per minute. This cadence prevents gastric insufflation and barotrauma.
The One-Person E-C Clamp Technique
The E-C clamp technique is the gold standard for solo manual ventilation. Place your thumb and index finger in a C shape over the mask to exert downward pressure. Hook the remaining three fingers under the mandible in an E shape. Pull the jaw up into the mask rather than pushing the mask down onto the face. This action maintains the airway and creates a superior seal. It's a high-fatigue move. Switch hands if your grip strength fades after two minutes of continuous use.
The Two-Person Technique (Tactical Best Practice)
Transition to a two-person technique whenever manpower allows. It's the most effective way to overcome seal leaks caused by thick beards or significant facial trauma, which can reduce seal efficacy by over 30 percent. The primary operator uses the thenar eminence grip, placing the palms on both sides of the mask for maximum downward pressure. Refining your critical care BVM use ensures the lead medic can focus solely on chest rise while the partner manages the bag. This division of labor increases tidal volume consistency.
Adjusting for the Tactical Environment
Tactical environments complicate basic procedures. Low-light conditions make visual chest rise assessment impossible. You must keep your hand on the casualty's chest to feel the expansion. Tactical gloves reduce tactile sensitivity by roughly 20 percent, so increase your grip focus. During extraction, secure the mask with a head strap to prevent displacement during high-speed movement. If operating in a CBRN environment, ensure the bag valve mask is equipped with a high-efficiency particulate air (HEPA) filter to protect the casualty and the team. This bag valve mask configuration is mandatory for prolonged field care in contaminated zones.
- Check the Seal: Listen for air escaping around the mask edges.
- Verify Airway: Ensure the OPA or NPA hasn't shifted during movement.
- Oxygenation: Connect to 15LPM oxygen if the mission profile allows for tanks.
Critical Troubleshooting: Overcoming Common BVM Failure Points
Tactical environments degrade clinical performance. Under the high-stress conditions of a Point of Injury intervention, the bag valve mask is often misused. The primary error is over-ventilation. Adrenaline drives operators to squeeze the bag too fast and too hard. This increases intrathoracic pressure, which directly reduces venous return to the heart. In a trauma patient already suffering from hypovolemia, this drop in preload can trigger immediate cardiac arrest. You must maintain a disciplined rate of 10 to 12 breaths per minute, or one squeeze every five to six seconds. Deliver each breath over one full second to minimize pressure spikes.
Equipment failure is a reality in rugged terrain. Blood, vomit, or field debris can clog the non-rebreathing valve, making ventilation impossible. Inspect the duck-bill valve for obstructions if you feel unusual resistance. Bag tears from jagged gear or sub-zero temperatures can also compromise the system. If the bag doesn't reinflate quickly, check the intake valve at the base for mud or snow blockages. Always carry a spare mask or a pocket BVM in your kit to ensure redundancy when your primary device fails.
Breath stacking, or air trapping, occurs when the patient doesn't have enough time to exhale fully. This is common in patients with underlying obstructive lung disease or during rapid, panicked bagging. It leads to barotrauma and decreased gas exchange. If you notice the chest isn't falling completely between squeezes, pause for two seconds to allow for full exhalation. Adjust your rhythm to match the patient's physiological requirements, not your own heart rate.
Gastric Insufflation and Aspiration Risks
Excessive pressure forces air past the esophageal sphincter and into the stomach. This typically happens when airway pressures exceed 20 cm H2O. Gastric distension pushes the diaphragm upward, further restricting lung expansion. It also makes vomiting nearly inevitable. Aspiration of gastric contents carries a 30 percent mortality rate in tactical settings. While the Sellick maneuver was once a standard intervention, current evidence suggests it's often ineffective. Focus instead on maintaining a superior seal and using slow, controlled volumes to keep air out of the gut.
The 'DOPE' Mnemonic for Tactical Troubleshooting
When ventilation becomes difficult or the patient's status deteriorates, use the DOPE mnemonic to identify the cause. This standardized approach prevents cognitive tunnel vision during a crisis.
- Displacement: Check if the mask has shifted or if the advanced airway has moved.
- Obstruction: Look for blood, broken teeth, or the tongue blocking the airway. Suction the oropharynx immediately.
- Pneumothorax: Assess for tension pneumothorax. Look for unequal chest rise or increased resistance. Perform needle decompression if indicated.
- Equipment: Verify the O2 supply is flowing and the bag valve mask valves are functioning without debris.
Master the skills required to manage complex airway failures by exploring our advanced medical training kits designed for the modern operator.
Integrating the BVM into Your Tactical Medical Kit
Selecting a bag valve mask for a tactical loadout requires balancing clinical capability with the severe spatial constraints of an IFAK or medic bag. High-performance medical gear outfitters prioritize equipment that withstands extreme temperature fluctuations and mechanical pressure. A standard BVM is often too bulky for individual kits, which leads some operators to omit this critical tool. This is a dangerous oversight in environments where prolonged field care or respiratory failure is a known risk. Your gear must be rugged enough to survive a HALO jump or a maritime insertion without losing seal integrity.
The Pocket BVM: The Operator's Choice
The Pocket BVM has become the industry standard for tactical units due to its collapsible design. While a standard unit occupies approximately 4,000 cubic centimeters of space, a collapsed pocket version fits into a ruggedized case the size of a hockey puck. You can achieve deployment from case to casualty in under 10 seconds with minimal practice. The Pocket BVM reduces storage footprint by up to 75% without sacrificing clinical function. This efficiency allows medics to carry a full resuscitation suite in a standard double-mag pouch or a small utility pocket on a plate carrier.
Essential BVM Accessories
A bag valve mask is only effective when the airway is patent. You must carry Oropharyngeal (OPA) and Nasopharyngeal (NPA) airways as primary adjuncts to prevent tongue occlusion during ventilation. Ensure your kit includes oxygen tubing and universal adapters for portable cylinder compatibility. Before addressing the airway, always follow MARCH protocols and consult bleeding control guidelines to ensure massive hemorrhage is mitigated first. Airway management is secondary to stopping life-threatening bleeds in the tactical environment.
Maintenance is a non-negotiable aspect of readiness. Inspect your gear every 90 days for signs of dry rot or seal degradation. In environments exceeding 110 degrees Fahrenheit, this inspection window should shorten to every 30 days. If the bag feels tacky or shows visible cracks, replace it immediately. Rubber components can become brittle, leading to catastrophic failure during a rescue attempt. Training must mirror these realities. High-fidelity simulation using manikins that provide real-time feedback on tidal volume and lung compliance is the only way to build the muscle memory required for effective manual ventilation under fire. Adhering to CoTCCC standards ensures your interventions remain evidence-based and effective when the mission dictates.
- Standard BVM: Best for vehicle kits and casualty collection points.
- Pocket BVM: Preferred for IFAKs and low-profile operations.
- Inspection: Check for seal integrity and valve function quarterly.
- Simulation: Practice one-handed and two-handed seal techniques under stress.
Mastering Airway Intervention in High-Threat Environments
Proficiency with the bag valve mask is a core competency that separates capable operators from the rest. You've explored the critical mechanics of manual ventilation and the specific troubleshooting steps needed to overcome equipment failure in the field. Adhering to established TCCC protocols ensures that your airway interventions remain effective under the physiological stress of a tactical engagement. It's not enough to carry the gear; you must master the seal and the stroke to maintain oxygenation when every breath is a battle. Since 2004, our veteran-owned and operated team has provided the hardware necessary for these exact scenarios. We supply government agencies and specialized units worldwide with field-proven gear that's been vetted by TCCC instructors. Reliability isn't a luxury in a crisis. It's a requirement for survival. Your commitment to training ensures you're ready when the call comes. Equip your kit with professional-grade BVMs and airway gear at MED-TAC to ensure your equipment is as ready as you are. Stay sharp, stay prepared, and keep your focus on the mission ahead.
Frequently Asked Questions
Can a bag valve mask be used on a conscious patient?
You shouldn't use a bag valve mask on a conscious casualty because it triggers the gag reflex and increases the risk of aspiration. Reserve manual ventilation for patients with a Glasgow Coma Scale score below 8 or those in respiratory arrest. If the casualty is awake, they'll fight the mask and cause gastric distention. Monitor the airway and use supplemental oxygen via a non-rebreather mask instead.
How do I know if I am over-ventilating the casualty?
You'll know you're over-ventilating if you see the casualty's abdomen distending or if their heart rate drops due to increased intrathoracic pressure. Deliver one breath every 6 seconds to avoid barotrauma; excessive ventilation reduces venous return to the heart. This can decrease survival rates by 30 percent in cardiac arrest scenarios. Focus on visible chest rise rather than squeezing the entire bag volume.
What is the correct ventilation rate for an adult in cardiac arrest?
The correct ventilation rate for an adult in cardiac arrest is 1 breath every 6 seconds, totaling 10 breaths per minute. This standard follows the 2020 AHA Guidelines for CPR and Emergency Cardiovascular Care. If you haven't established an advanced airway, maintain a 30:2 compression-to-ventilation ratio. Deliver each breath over 1 second to ensure adequate oxygenation without compromising the casualty's circulatory flow.
Do I need to be a doctor to use a BVM in an emergency?
You don't need to be a doctor to use this device, but you must have formal training in airway management and ventilation. Certified First Responders, EMTs, and Combat Medics utilize these tools regularly under TCCC protocols. State laws and local EMS regulations define the specific scope of practice for non-physicians. Ensure you've completed a BLS or ACLS course to master the E-C clamp technique.
Can I use a BVM without an oxygen tank?
You can use a bag valve mask without an oxygen tank to deliver room air at a 21 percent oxygen concentration. While supplemental oxygen is preferred to reach 90 percent or higher concentrations, manual ventilation remains effective for moving air into the lungs. In tactical environments, you'll often rely on ambient air until a CASEVAC platform arrives. Always attach the reservoir bag even when oxygen is unavailable.
What should I do if the casualty starts vomiting while using a BVM?
If the casualty starts vomiting, immediately turn them onto their side in the recovery position and clear the airway. Use a portable suction unit or a manual sweep to remove all debris. Failure to clear the airway before resuming ventilation will force gastric contents into the lungs, leading to aspiration pneumonia. Once the airway is clear, resume the MARCH algorithm and continue providing respiratory support.
How often should I replace the BVM in my trauma kit?
Replace the unit in your trauma kit every 5 years or according to the manufacturer's expiration date. Environmental stressors like heat in a vehicle or kit can degrade the silicone and plastic valves faster than expected. Inspect your gear every 30 days for cracks or loss of seal integrity. If you've used the device on a casualty, dispose of it immediately as these are single-use medical items.
Is a Pocket BVM as effective as a full-sized Ambu bag?
A Pocket BVM is as effective as a full-sized Ambu bag, providing the same 1600ml stroke volume in a compact form factor. This ruggedized version fits into a standard 4.5-inch diameter case, saving 75 percent more space in an IFAK or medic bag. It meets all standard ISO requirements for manual resuscitators. The collapsible design doesn't compromise the clinical performance required for life-saving respiratory support in the field.
Leave a comment